Cms L564 Printable Form
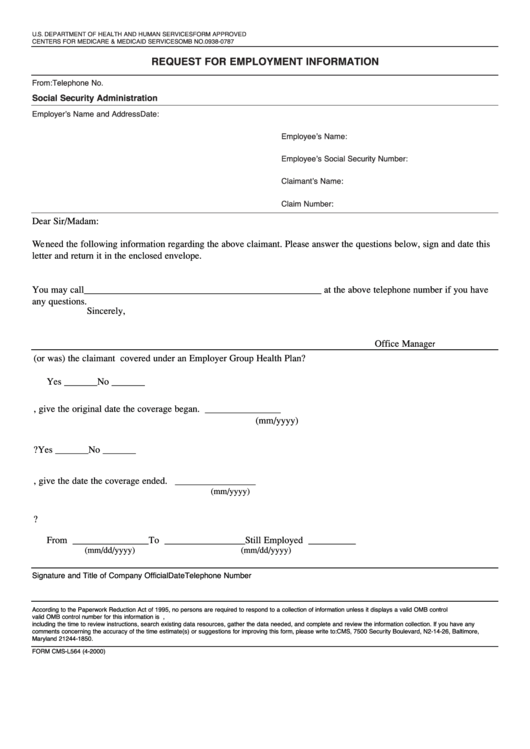
Cms L564 Printable Form - If you have questions, call. Use get form or simply click on the template preview to open it in. Easily fill out pdf blank, edit, and sign them. You can use this form to sign up for part b: • your basic information and employer name other important information: Web this form is your application for medicare part b (medical insurance). Web this form is used for proof of group health care coverage based on current employment. Web what you’ll need: Web find and fill out the correct form cms l564 printable. It’s used in conjunction with form. Department of health and human services centers for medicare. Web what’s the form called? • your basic information and employer name other important information: Web what you’ll need: If you have questions, call. • your basic information and employer name other important information: Web quick steps to complete and design cm's l564 form online: This information is needed to process your. • your employer will need to complete the second half of the form with your employment dates and dates of your group health plan coverage. Web this form is used for proof. Use get form or simply click on the template preview to open it in. Web this form is used for proof of group health care coverage based on current employment. You can use this form to sign up for part b: It’s used in conjunction with form. Web find and fill out the correct form cms l564 printable. If you have questions, call. Web find and fill out the correct form cms l564 printable. If you have medicare part a (hospital insurance) and you’re eligible to. Easily fill out pdf blank, edit, and sign them. Web what’s the form called? Web this form is used for proof of group health care coverage based on current employment. You can use this form to sign up for part b: • your employer will need to complete the second half of the form with your employment dates and dates of your group health plan coverage. If you have questions, call. Web what you’ll. This information is needed to process your. Web what you’ll need: Easily fill out pdf blank, edit, and sign them. If you have medicare part a (hospital insurance) and you’re eligible to. Web what’s the form called? If you have medicare part a (hospital insurance) and you’re eligible to. Web quick steps to complete and design cm's l564 form online: If you have questions, call. Web what’s the form called? • your basic information and employer name other important information: If you have questions, call. Easily fill out pdf blank, edit, and sign them. Web this form is used for proof of group health care coverage based on current employment. Web quick steps to complete and design cm's l564 form online: • your basic information and employer name other important information: • your basic information and employer name other important information: It’s used in conjunction with form. Department of health and human services centers for medicare. Web this form is used for proof of group health care coverage based on current employment. If you have medicare part a (hospital insurance) and you’re eligible to. • your basic information and employer name other important information: Department of health and human services centers for medicare. Web quick steps to complete and design cm's l564 form online: Easily fill out pdf blank, edit, and sign them. Web this form is used for proof of group health care coverage based on current employment. Web what you’ll need: Web this form is your application for medicare part b (medical insurance). Web quick steps to complete and design cm's l564 form online: Web what’s the form called? Use get form or simply click on the template preview to open it in. Web this form is used for proof of group health care coverage based on current employment. Easily fill out pdf blank, edit, and sign them. You can use this form to sign up for part b: Department of health and human services centers for medicare. If you have medicare part a (hospital insurance) and you’re eligible to. • your basic information and employer name other important information: Web find and fill out the correct form cms l564 printable. If you have questions, call. It’s used in conjunction with form. • your employer will need to complete the second half of the form with your employment dates and dates of your group health plan coverage. This information is needed to process your.
Medicare Part B Enrollment Form Cms L564 Form Resume Examples

Social Security Tax Form 1099 Universal Network
Application For Medicare Part B Employer Form Form Resume Examples
Application For Medicare Part B Employer Form Form Resume Examples
Form CmsL564 Request For Employment Information, Medicare True/false

Medicare Part B Application Form Cms L564 Form Resume Examples
Form CmsL564 Request For Employment Information printable pdf download
20162021 Form CMSL564 Fill Online, Printable, Fillable, Blank pdfFiller

Cms L564 Printable Form Master of Documents
Top Cms 1450 Form Templates free to download in PDF format
Related Post: